quadrantanopia
[kwod″ran-tah-no´pe-ah]defective vision or blindness in one fourth of the visual field.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
qua·drant·an·o·pi·a
(kwah'drant-an-ō'pē-ă),Loss of vision in a quarter section of the visual field of one or both eyes; if bilateral, it may be homonymous or heteronymous, binasal or bitemporal, or crossed, for example, involving the upper quadrant in one eye and the lower quadrant in the other.
Synonym(s): quadrantic hemianopia
Farlex Partner Medical Dictionary © Farlex 2012
quadrantanopia
Visual field loss in a quarter of the visual field of the eye. The defect is usually bilateral, as it is caused by a lesion past the optic chiasma. It may be homonymous (binasal, bitemporal, upper or lower), crossed (one upper and the other lower), congruous (equal size of the defects), or incongruous (unequal size of the defects) (Fig. Q1). Syn. quadrantanopsia; quadrantic anopsia; quadrantic hemianopia. See hemianopia.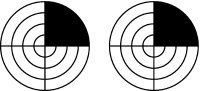

)
Fig. Q1 Complete, right, superior homonymous quadrantanopia due to a lesion of the optic radiations in the left temporal lobe
Millodot: Dictionary of Optometry and Visual Science, 7th edition. © 2009 Butterworth-Heinemann