Breast cancer
Definition
Breast cancer is caused by the development of malignant cells in the breast. The malignant cells originate in the lining of the milk glands or ducts of the breast (ductal epithelium), defining this malignancy as a cancer. Cancer cells are characterized by uncontrolled division leading to abnormal growth and the ability of these cells to invade normal tissue locally or to spread throughout the body, in a process called metastasis.
Description
Breast cancer arises in the milk-producing glands of the breast tissue. Groups of glands in normal breast tissue are called lobules. The products of these glands are secreted into a duct system that leads to the nipple. Depending on where in the glandular or ductal unit of the breast the cancer arises, it will develop certain characteristics that are used to sub-classify breast cancer into types. The pathologist will note the subtype at the time of evaluation with the microscope. Ductal carcinoma begins in the ducts, lobular carcinoma has a pattern involving the lobules or glands. The more important classification is related to the evaluated tumor's capability to invade, as this characteristic defines the disease as a true cancer. The stage before invasive cancer is called in situ, meaning that the early malignancy has not yet become capable of invasion. Thus, ductal carcinoma in situ is considered a minimal breast cancer.
How breast cancer spreads
The primary tumor begins in the breast itself, but once it becomes invasive, it may progress beyond the breast to the regional lymph nodes or travel (metastasize) to other organ systems in the body and become systemic in nature. Lymph is the clear, protein-rich fluid that bathes the cells throughout the body. Lymph will work its way back to the bloodstream via small channels known as lymphatics. Along the way, the lymph is filtered through cellular stations known as nodes, thus they are called lymph nodes. Nearly all organs in the body have a primary lymph node group filtering fluid that comes from that organ. In the breast, the primary lymph nodes are under the armpit, or axilla. Classically, the primary tumor begins in the breast and the first place to which it is likely to spread is the regional lymph nodes. Cancer, as it invades in its place of origin, may also work its way into blood vessels. If cancer gets into the blood vessels, the blood vessels provide yet another route for the cancer to spread to other organs of the body.
Breast cancer follows this classic progression though it often becomes systemic or widespread early in the course of the disease. By the time one can feel a lump in the breast it is often 0.4 inches, or one centimeter, in size and contains roughly a million cells. It is estimated that a tumor of this size may take one to five years to develop. During that time, the cancer may metastasize, or spread by lymphatics or blood to areas elsewhere in the body.
When primary breast cancer spreads, it may first go to the axillary nodes. If this occurs, regional metastasis exists. If it proceeds elsewhere either by lymphatic or blood-borne spread, the patient develops systemic metastasis that may involve a number of other organs in the body. Favorite sites of systemic involvement for breast cancer are the lung, bones, liver, skin, and soft tissue. As it turns out, the presence of, and the actual number of, regional lymph nodes containing cancer remains the single best indicator of whether or not the cancer has become widely metastatic. Because tests to discover metastasis in other organs may not be sensitive enough to reveal minute deposits of cancer cells, the evaluation of the axilla for regional metastasis becomes very important in making treatment decisions for this disease.
If breast cancer spreads to other major organs of the body, its presence will compromise the function of those organs. Death is the result of extreme compromise of vital organ function.
Demographics
Every woman is at risk for breast cancer. If she lives to be 85, there is a one in eight chance (12%) that she will develop breast cancer sometime during her life. As a woman ages, her risk of developing breast cancer rises dramatically regardless of her family history. The breast cancer risk of a 25-year-old woman is only one out of 19,608; by age 45, it is one in 93. In fact, fewer than 5% of cases are discovered before age 35 and the majority of all breast cancers are found in women over age 50.
In 2008, about 182,500 new cases of breast cancer and 67,800 cases of cancer in situ were diagnosed in the United States. About 40,000 women die of breast cancer each year; breast cancer is the second leading cause of cancer death in women. However, in the United States, there 2.5 million breast cancer survivors. Deaths from breast cancer are declining in recent years, a reflection of earlier diagnosis from screening mammograms, improving therapies and a dramatic decrease in the use of hormone replacement therapy (HRT) in post-menopausal women.
Causes and symptoms
All cancer is thought to occur because of small changes (mutations) in genes. A gene is a small packet of deoxyribonucleic acid (DNA), the genetic master molecule of all cells that is inherited from each parent. Genes control all aspects of development and metabolism. Small changes in the structure of genes can cause changes in proteins that regulate metabolic functions. In healthy cells, cell division is controlled by proteins regulated by genes. Specific genes make proteins that signal healthy cells when to stop dividing. In cancer, the controlling gene(s) is damaged or mutated and does not produce the proteins necessary to signal cells to stop dividing. The mutations that cause breast cancer do not have a single cause. Genetic, environmental, and lifestyle factors all play a role in determining who gets breast cancer. Although men can get breast cancer, women are 100 times more likely to develop the disease.
There are a number of risk factors for the development of breast cancer; however, among experts there is some disagreement about how important each of these factors is. Risk factors include:
- age. Eighty % of breast cancers are found in women over age 50.
- a family history of breast cancer in mother or sister.
- carrying the BRCA1 and BRCA2 genes. Women with these genes account for 5-10% of breast cancer cases and have an 80% chance of developing breast cancer at some time during their life.
- history of abnormal breast biopsies or previous history of breast cancer.
- having first menstruation before age 12 or entering menopause after age 55.
- having no children or having a first child after age 30.
- daily alcohol consumption of two drinks or more.
- obesity and a high fat diet.
- breast exposure to radiation (e.g., in treatment of other cancers).
- postmenopausal hormone replacement therapy (HRT) with a combination estrogen/progesterone drug. Estrogen alone does not appear to increase risk. The longer a woman used HRT, the more her risk increases.
HRT provides significant relief of menopausal symptoms, prevention of osteoporosis, and possibly protection from cardiovascular disease and stroke. While physicians have long known a small increased risk for breast cancer was linked to use of HRT, a landmark study released in 2003 proved the risk was greater than thought. The Women's Health Initiative found that even relatively short-term use of estrogen plus progestin is associated with increased risk of breast cancer, diagnosis at a more advanced stage of the disease, and a higher number of abnormal mammograms.
Of all the risk factors listed above, family history is the most important. Some studies have found that about half of all familial breast cancer cases (families in which there is a high breast cancer frequency) have mutations affecting the genes BRCA-1 or BRCA-2. Other genes (e.g., ATM, CHEK2, p53, PTEN) have been identified that may influence the development of breast cancer, but their impact is much less than the BRCA genes. Nevertheless, breast cancer due to heredity is only a small proportion of breast cancer cases; only 5%-10% of all breast cancer cases will be women who inherited a high susceptibility through their genes.
Although there are many recognized risk factors, it is important to note that more than 70% of women who get breast cancer have no known risk factors. Having several risk factors may increase a woman's chance of developing breast cancer, but the interplay of predisposing factors is complex. In addition to those accepted factors listed above, some studies suggest that high-fat diets, obesity, or the use of alcohol may contribute to the risk profile.
Not all lumps detected in the breast are cancerous. Fibrocystic changes in the breast are extremely common. Also known as fibrocystic condition of the breast, fibrocystic changes are a leading cause of non-cancerous lumps in the breast. Fibrocystic changes also cause symptoms of pain, swelling, or discharge and may become evident to the patient or physician as a lump that is either solid or filled with fluid. Complete diagnostic evaluation of any significant breast abnormality is mandatory because, although women commonly develop fibrocystic changes, breast cancer is common also, and the signs and symptoms of fibrocystic changes overlap with those of breast cancer. Certain benign changes in the breast may now be linked to increased risk for breast cancer.
Diagnosis
The diagnosis of breast cancer is accomplished by the biopsy of any suspicious lump or mammographic abnormality that has been identified. (A biopsy is the removal of tissue for examination by a pathologist. A mammogram is a low-dose, 2-view, x-ray examination of the breast.) The patient may be prompted to visit her doctor upon finding a lump in a breast, or she may have noticed skin dimpling, nipple retraction, or discharge from the nipple. A patient may not have noticed a symptom or abnormality, before a lump was detected by a screening mammogram.
When a patient has no signs or symptoms
Screening involves the evaluation of women who have no symptoms or signs of a breast problem. Mammography has been helpful in detecting breast cancer that cannot be identified on physical examination. More than 90% of all breast cancers are detected by mammogram screening. However, about 10% of breast cancer does not show up on mammography, and a similar number of patients with breast cancer have an abnormal mammogram and a normal physical examination. These figures emphasize the need for regular examination as part of the screening process.
Screening
All women are encouraged to do regular, monthly breast self-examinations. This involves feeling the breasts for any abnormal lumps or pain. If an uncertainty or a lump is found, evaluation by an experienced physician and a mammogram is recommended. The American Cancer Society (ACS) has made recommendations for the use of mammography on a screening basis. In 2009, the ACS guidelines recommended that women should begin annual screening at age 40 For women at high risk for breast cancer, the ACS recommends beginning screenings at an earlier age, having screening at more frequent intervals, and having magnetic resonance imaging (MRI) screening in addition to a standard mammogram. A list of conditions considered to put women at high risk for breast cancer can be found on the ACS Web site.
Because of the greater awareness of breast cancer in recent years, screening evaluations by examinations and mammography are performed much more frequently than in the past. As a result, the number of breast cancers diagnosed has increased, but the disease is being diagnosed at an earlier stage than previously. The earlier the stage of disease at the time it is discovered, the better the long-term outcome (prognosis) becomes.
When a patient has physical signs or symptoms
A common finding that leads to diagnosis is the presence of a lump within the breast. Skin dimpling, nipple retraction, or discharge from the nipple are less frequent initial findings prompting biopsy. Though bloody nipple discharge is distressing, it is most often caused by benign disease. Skin dimpling or nipple retraction in the presence of an underlying breast mass on examination is a more advanced finding. Actual skin involvement, with swelling (edema) or ulceration of the skin, are late findings.
The presence of a breast lump is a common sign of breast cancer. If the lump is suspicious and the patient has not had a mammogram by this point, a study should be done on both breasts prior to anything else so that the original characteristics of the lesion can be studied. The opposite breast should also be evaluated mammographically to determine if other problems exist that were undetected by physical examination.
Whether an abnormal screening mammogram or one of the signs mentioned above followed by a mammogram prompted suspicion, the diagnosis is established by obtaining tissue by biopsy of the area. There are different types of biopsy, each used with its own indication. If signs of widespread metastasis are already present, biopsy of the metastasis itself may establish diagnosis.
Biopsy
Depending on the situation, different types of biopsy may be performed. The types include incisional and excisional biopsies. In an incisional biopsy, the physician takes a sample of tissue, and in excisional biopsy, the mass is removed. Fine needle aspiration biopsy and core needle biopsy are kinds of incisional biopsies.
Fine needle aspiration biopsy
In a fine needle aspiration biopsy, a fine-gauge needle may be passed into the lesion and cells from the area suctioned into the needle can be quickly prepared for microscopic evaluation (cytology). (The patient experiencing nipple discharge also can have a sample taken of the discharge for cytological evaluation.) Fine needle aspiration is a simple procedure that can be done under local anesthesia, and will tell if the lesion is a fluid-filled cyst or whether it is solid. The sample obtained will yield much diagnostic information. Fine needle aspiration biopsy is an excellent technique when the lump is palpable and the physician can easily hit the target with the needle. If the lesion is a simple cyst, the fluid will be evacuated and the mass will disappear. If it is solid, the diagnosis may be obtained. Care must be taken, however, because if the mass is solid and the specimen is non-malignant, a complete removal of the lesion may be appropriate to be sure.
Core needle biopsy
Core needle biopsies also are obtained simply under local anesthesia. The larger piece of tissue obtained with its preserved architecture may be helpful in confirming the diagnosis short of open surgical removal. An open surgical incisional biopsy is rarely needed for diagnosis because of the needle techniques. If there remains question as to diagnosis, a complete open surgical biopsy may be required.
Excisional biopsy
When performed, the excisional (complete removal) biopsy is a minimal outpatient procedure often done under local anesthesia.
Non-palpable lesions
As screening increases, non-palpable lesions (abnormalities that can not be felt by hand examination) demonstrated only by mammography are becoming more common. The use of x rays and computers to guide the needle for biopsy or to place markers for the surgeon performing the excisional biopsy are commonly employed. Some benign lesions can be fully removed by multiple directed core biopsies. These techniques are very appealing because they are minimally invasive; however, the physician needs to be careful to obtain a good sample.
Other tests
If a lesion is not palpable and has simple cystic characteristics on mammography, ultrasound may be used both to determine that it is a cyst and to guide its evacuation. Ultrasound may also be used in some cases to guide fine needle or core biopsies of the breast.
Computed tomography (CT) scans are used only rarely in the evaluation of breast lesions. MRI is recommended for high-risk women and to follow up on suspicious findings from mammograms or for certain patients.
Treatment
Staging
Once diagnosis is established and before treatment is begun, more tests are done to determine if the cancer has spread beyond the breast. These tests include a chest x ray and blood count with liver function tests. Along with the liver function measured by the blood sample, the level of alkaline phosphatase, an enzyme from bone, is also determined. A radionuclear bone scan may be ordered. This test looks at the places in the body to which breast cancer usually metastasizes. A CT scan also may be ordered. The physician will do a careful examination of the axillae to assess likelihood of regional metastasis. Sometimes, the physician will remove all of the axillary lymph nodes to assess breast cancer stage. However, recent studies show great success with sentinel lymph node biopsy. This technique removes the sentinel lymph node, or that lymph node that receives fluid drainage first from the area where the cancer is located. If this node is free of cancer, staging can be assigned accordingly. This method saves women the discomfort and side effects associated with removing additional lymph nodes in her armpit.
Using the results of these studies, the stage of cancer is defined for the patient. This helps establish a treatment protocol and prognosis. In the United States, formal staging is done using the TNM system. This system considers the tumor size and how much it has grown (T), whether the cancer has spread to the lymph nodes (N), and whether it has metastasized (M) to distant sites in the body. Stages are summarized below.
- Stage I. The cancer is no larger than 2 cm and no cancer cells are found in the lymph nodes.
- Stage II. The cancer is no larger than 2 cm but has spread to the lymph nodes or is larger than 2 cm but has not spread to the lymph nodes.
- Stage IIIA. Tumor is larger than 5 cm and has spread to the lymph nodes or is smaller than 5 cm, but has spread to the lymph nodes, which have grown into each other.
- Stage IIIB. Cancer has spread to tissues near the breast or to lymph nodes inside the chest wall, along the breastbone.
- Stage IV. Cancer has spread to skin and lymph nodes near the collarbone or to other organs of the body.
Treatment
Surgery, radiation, and chemotherapy all may be used in the treatment of breast cancer. Depending on the stage, they will be used in different combinations or sequences to effect an appropriate strategy for the type and stage of the disease being treated.
Surgery
Historically, surgical removal of the entire breast and axillary lymph nodes, along with the muscles down to the chest wall (radical mastectomy), was performed as the preferred therapy for breast cancer. In the past 30 years, surgery remains a primary option, but other therapies have risen in importance. Recent studies have suggested that breast conserving treatment (as opposed to radical mastectomy) improves the quality of life for women without compromising survival. Ultimately, the extent of surgery depends on the type of breast cancer, whether the disease has spread, and the patient's age and health.
If the tumor is less than 1.5 (4 cm) in size and located so that it can be removed without destroying the reasonable cosmetic appearance of the residual breast, just the primary tumor and a rim of normal tissue will be removed. The axillary nodes will still be removed for staging purposes, usually through a separate incision. Because of the risk of recurrence in the remaining breast tissue, radiation therapy is used to lessen the chance of local recurrence. This type of primary therapy is known as lumpectomy, (or segmental mastectomy), and axillary dissection.
Sentinel lymph node biopsy, a technique for identifying which nodes in the axilla drain the tumor, has been developed to provide selective sampling and further lessen the degree of surgical trauma the patient experiences.
When patients are selected appropriately based on the preoperative clinical stage, all of these surgical approaches have been shown to produce similar results. In planning primary surgical therapy, it is imperative that the operation is tailored to fit the clinical circumstance of the patient.
The pathologic stage of the cancer is evaluated after surgical treatment and defines additional treatment. In addition to stage, other tests may be necessary to aid in decisions regarding additional adjuvant therapies. Adjuvant therapies are treatments used after the primary treatment to help ensure that no microscopic disease exists and to help prolong patients' survival time or reduce pain.
Radiation therapy
Like surgical therapy, radiation therapy is a local modality-it treats only the specific tissue exposed to radiation and not the rest of the body. Radiation is usually given post-operatively after surgical wounds have healed. The pathologic stage of the primary tumor is now known and this aids in treatment planning. The extent of the local surgery also influences the planning. Radiation may not be needed at all after modified radical mastectomy for stage I disease but is usually used when breast-preserving surgery is performed. If the tumor was extensive or if multiple nodes were involved, the field of tissue exposed will vary accordingly. Radiation is used as an adjunct to surgical therapy and is considered important to gaining local control of the tumor. In the past, radiation was used as an alternative to surgery on occasion. However, now that breast-preserving surgical protocols have been developed, primary radiation treatment of the tumor is no longer performed. Radiation also has an important role in the treatment of the patient with widespread (disseminated) disease, particularly if it involves the skeleton. Radiation therapy can affect pain control and prevention of fracture in this circumstance.
Chemotherapy
Survival after breast cancer surgery is improved by the addition of postoperative chemotherapy. Post-surgical chemotherapy therapy in patients who have no evidence of residual disease is now performed on the basis that some patients have metastases that are too small to be detectable. This occurs because it is unlikely that the surgeon has removed every single cancerous cell. Loose cancer cells, if not killed by chemotherapy, may travel through the circulatory system and form new tumors elsewhere. Chemotherapy may also be given in some circumstances before surgery. Chemotherapy is administered either orally or by injection into a blood vessel and usually involves multiple drugs. It is given in cycles, followed by a period of time for recovery, followed by another course of drugs.
Chemotherapy can produce significant side effects, including nausea and vomiting, temporary hair loss, mouth or vaginal sores, fatigue, weakened immune system, and infertility. Complementary therapies are often helpful in reducing some of these side effects.
Hormone therapy
Many breast cancers, particularly those originating in post-menopausal women, are responsive to hormones. These cancers have receptors on their cells for the hormone estrogen. Part of the post-surgery primary tumor assessment is evaluation for the presence of estrogen and progesterone receptors. If they are present on the cancer cells, altering the hormone status of the patient will slow tumor growth and have a positive impact on survival. Hormonal status may be changed with drug therapy. The drug tamoxifen binds to estrogen receptors on the cancer cells, so that hormones cannot interact with the cells and stimulate their growth. If the patient has these receptors present, tamoxifen is commonly prescribed for five years as an adjunct to primary treatment. In women whose cancer cells have estrogen receptors, tamoxifen reduces the chance of breast cancer reoccurring by about 50%.
Toremifene (Fareston) and fulvestrant (Faslodex) are drugs similar to tamoxifen in that they target hormone receptors on cancer cells. They are often used when cancer cells are unresponsive to tamoxifen. In addition, a new group of drugs called aromatase inhibitors that block the enzymes that produce estrogen in postmenopausal (but not premenopausal) women have been used to treat both early and late advanced breast cancer. These drugs include drugs are letrozole (Femara), anastrozole (Arimidex), and exemestane (Aromasin). Because of these agents, there is rarely any need for surgical removal of hormone-producing glands, such as the ovary or adrenal, that was sometimes necessary in the past.
Biotherapeutics
Biotherapeutics are a type of targeted therapy. Large amounts of antibodies of a single type (called monoclonal antibodies) that react with specific receptors on cancer cells are made in the laboratory. When given to the patient, they inactivate or destroy those cells containing that specific receptor, but do not react with other cells. Trastuzumab (Herceptin) and Lapatinib (Tykerb) target cells that contain a growth protein known as HER/2. Between 15% and 25% of women have breast cancer that responds to these drugs. Bevacizumab (Avastin) is a biotherapeutic used to treat breast cancer that has metastasized. It helps prevent tumors from becoming established by interfering with the growth of blood vessels into the tumor. Without access to nutrients in the blood, the tumors cannot increase in size. Biotherapeutics are normally used in addition to chemotherapy drugs.
Complementary adjuvant therapy
Complementary treatments used along with conventional medicine are often successful in moderating side effects and improving the patient's quality of life. For example, acupuncture and guided imagery may be useful tools in treating pain symptoms and side effects of chemotherapy associated with breast cancer. Acupuncture involves the placement of a series of thin needles into the skin at targeted locations on the body, known as acupoints, in order to harmonize the energy flow within the human body. Guided imagery involves creating a visual mental image of pain. Once the pain can be visualized, the patient can adjust the image to make it more pleasing, and thus more manageable.
Many herbal remedies are available to lessen pain symptoms and chemotherapy side effects such as nausea, and to promote relaxation and healing. However, breast cancer patients should consult with their healthcare professional before taking any herbal treatments. Depending on the preparation and the type of herb, these remedies may interact with and enhance or diminish the effects of other prescribed medications. One herb that is generally regarded as helpful in relieving the nausea that accompanies chemotherapy, is ginger (Zingiber officinale).
Prognosis
The prognosis for breast cancer depends on the type and stage of cancer. Lymph node involvement is one of the best indicators of breast cancer survival rates. According to the American Cancer Society, As of 2009, the five-year survival rate for American women with carcinoma in situ and stage I breast cancer was 100%. The five-year survival rate for women with stage II breast cancer 86% About 53% of stage III patients survive five years, and about 20% of stage IV patients do so.
Prevention
While breast cancer cannot be prevented, making lifestyle choices that eliminate the risk factors listed above is both prudent and promotes general health and well being. While regular breast exams and screening mammograms will not prevent breast cancer, they significantly aid in its early detection and treatment, thus increasing the chances of survival.
Key Terms
- Adjuvant therapy
- Treatment involving radiation, chemotherapy (drug treatment), or hormone therapy, or a combination of all three given after the primary treatment for the possibility of residual microscopic disease.
- Aneuploid
- An abnormal number of chromosomes in a cell.
- Aspiration biopsy
- The removal of cells in fluid or tissue from a mass or cyst using a needle for microscopic examination and diagnosis.
- Benign
- Not malignant, noncancerous.
- Biopsy
- A procedure in which suspicious tissue is removed and examined by a pathologist for cancer or other disease. For breast biopsies, the tissue may be obtained by open surgery, or through a needle.
- Hormones
- Chemicals produced by glands in the body that circulate in the blood and control the actions of cells and organs. Estrogens are hormones that affect breast cancer growth.
- Hormone therapy
- Treating cancers by changing the hormone balance of the body, instead of by using cell-killing drugs.
- Lumpectomy
- A surgical procedure in which only the cancerous tumor in the breast is removed, together with a rim of normal tissue.
- Lymph nodes
- Small, bean-shaped masses of tissue scattered along the lymphatic system that act as filters and immune monitors, removing fluids, bacteria, or cancer cells that travel through the lymph system. Breast cancer cells in the lymph nodes under the arm or in the chest are a sign that the cancer has spread, and that it might recur.
- Malignant
- Cancerous.
- Mammography
- X-ray imaging of the breast that can often detect lesions in the tissue too small or too deep to be felt.
- Oncogene
- A gene that has to do with regulation of cancer growth. An abnormality can produce cancer.
For Your Information
Resources
Books
- Link, John S. Breast Cancer Survival Manual: A Step-by-Step Guide for the Woman With Newly Diagnosed Breast Cancer, 4th ed. New York: H. Holt, 2007
- Miller, Kenneth D. Choices in Breast Cancer Treatment: Medical Specialists and Cancer Survivors Tell You What You Need to Know. Baltimore: Johns Hopkins University Press, 2008.
- "Breast Cancer." MedlinePlus. January 28, 2009 [cited January 29, 2009]. http://www.nlm.nih.gov/medlineplus/breastcancer.html.
- "Breast Cancer." Centers for Disease Control and Prevention. July 11, 2008 [cited January 28, 2009]. http://www.cdc.gov/cancer/breast.
- "What You Need to Know About Breast Cancer." National cancer Institute. November 1, 2007 [cited January 28, 2009]. http://www.cancer.gov/cancertopics/wyntk/breast.
- American Cancer Society. 1599 Clifton Road NE, Atlanta GA 30329-4251. Telephone: 800 ACS-2345. http://www.cancer.org.
- Breast Cancer Network of Strength Headquarters 212 W. Van Buren, Suite 1000, Chicago, IL 60607-3903. Telephone (office):(312) 986-8338. Breast Cancer Support Center: (800) 221-2141 (English) (800) 986-9505 (Espanol) Fax: (312)294-8597 http://www.networkofstrength.org.
- National Cancer Institute Public Inquiries Office. 6116 Executive Boulevard, Room 3036A, Bethesda, MD 20892-8322 . Telephone: (800) 4-CANCER. http://www.cancer.gov.
Cancer treatment
Cancer diagnosis
Hormone therapy
Breast biopsy
Breast cancer
Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.
breast
[brest]the front of the chest, especially the modified cutaneous, glandular structure it bears, the mamma. In women the breasts are secondary sex organs with the function of producing milk after childbirth. The term breast is less commonly used to refer to the breasts of the human male, which neither function nor develop.
At the tip of each breast is an area called the areola, usually reddish in color; at the center of this area is the nipple. About 20 separate lactiferous ducts empty into a depression at the top of the nipple. Each duct leads from alveoli within the breast called lobules, where the milk is secreted. Along their length, the ducts have widened areas that form reservoirs in which milk can be stored. The ducts and lobules form the glandular tissue of the breasts. Connective tissue covers the glandular tissue and is itself sheathed in a layer of fatty tissue. The fatty tissue gives the breast its smooth outline and contributes to its size and firmness.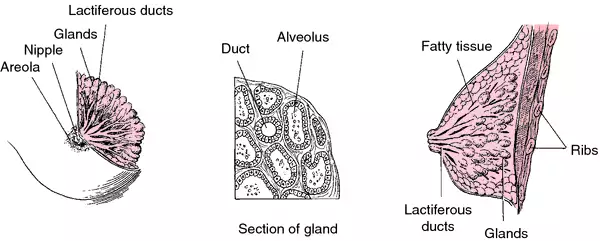
At the tip of each breast is an area called the areola, usually reddish in color; at the center of this area is the nipple. About 20 separate lactiferous ducts empty into a depression at the top of the nipple. Each duct leads from alveoli within the breast called lobules, where the milk is secreted. Along their length, the ducts have widened areas that form reservoirs in which milk can be stored. The ducts and lobules form the glandular tissue of the breasts. Connective tissue covers the glandular tissue and is itself sheathed in a layer of fatty tissue. The fatty tissue gives the breast its smooth outline and contributes to its size and firmness.

Breast, with detail and cross section.

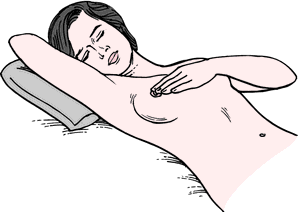
Breast self-examination. From Lowdermilk et at., 2000. 1. The best time to do breast self-examination is after your period, when breasts are not tender or swollen. If you do not have regular periods or sometimes skip a month, do it on the same day every month. 2. Lie down and put a pillow under your right shoulder. Place your right arm behind your head (Fig. 1). 3. Use the finger pads of your three middle fingers on your left hand to feel for lumps or thickening. Your finger pads are the top third of each finger. 4. Press firmly enough to know how your breast feels. If you're not sure how hard to press, ask your health care provider, or try to copy the way your health care provider uses the finger pads during a breast examination. Learn what your breast feels like most of the time. A firm ridge in the lower curve of each breast is normal. 5. Move around the breast in a set way. You can choose either circles (Fig. 2, A), vertical lines (Fig. 2, B), or wedges (Fig. 2, C€). Do it the same way every time. It will help you to make sure that you've gone over the entire breast area and to remember how your breast feels. 6. Gently compress the nipple between your thumb and forefinger and look for discharge. 7. Now examine your left breast using the finger pads of your right hand. 8. If you find any changes, see your health care provider right away. 9. You may want to check your breasts while standing in front of a mirror right after you do your breast self-examination each month. See if there are any changes in the way your breasts look: dimpling of the skin, changes in the nipple, or redness or swelling. 10. You may also want to do an extra breast self-examination while you're in the shower (Fig. 3). Your soapy hands will glide over the wet skin, making it easy to check how your breasts feel. 11. It is important to check the area between the breast and the underarm and the underarm itself. Also examine the area above the breast to the collarbone and to the shoulder.
Surgery of the Breast. Surgical operations of the breast are done for a variety of reasons. mammoplasty refers to reconstructive surgery of the breast and includes procedures to enlarge the breasts (augmentation mammoplasty), reduce their size (reduction mammoplasty), or reconstruct one or both breasts so that they are equal in size and contour. With the advent of less radical surgery for breast malignancies, postmastectomy plastic surgery of the breast has become more commonplace. mastectomy is surgical removal of breast tissue; it is most often done to treat breast cancer. Procedures can vary from a simple lumpectomy to a radical procedure in which the surgeon removes the internal mammary chain of lymph nodes, the entire breast, the underlying pectoral muscles, and the adjacent axillary lymph nodes.
breast cancer malignancy of the breast; it is second only to lung cancer as a cause of cancer deaths in North American women. It currently affects 1 in 9 women in the United States (11 per cent) and is called an epidemic by authorities. The incidence of breast cancer appears to be rising each year, even though when all age groups are considered its death rate has slightly declined in the past two decades. Risk factors include age over 40, close family member with breast cancer, onset of menses before age 13 or continuation beyond age 50, nulliparity, and first child after age 30.
Breast Self-Examination. Women should train themselves to perform a simple self-examination of the breasts (see illustration). The best time for this is just after menstruation when the breasts are normally soft. If any lump in the breast can be felt, a health care provider should be consulted immediately.
As with other forms of cancer, early detection and prompt treatment of malignancy of the breast are the keys to eradication of the disease. Studies have shown that breast self-examination has contributed to earlier detection and improved survival rates. It should be done monthly; more than 90 percent of breast cancers are discovered by the patients themselves either by chance or by routine self-examination. The American Cancer Society reports that only about 69 percent of women polled in the past had done self-examination at any time during the past year and less than 29 percent did it routinely each month.
Screening should begin by age 40 and should consist of a clinical examination every year and screening mammography every one or two years. Beginning at age 50, both the clinical examination and the mammography should be done once a year. mammography is considered to be the best diagnostic method for early detection when tumors are small and not readily found by palpation. Other diagnostic techniques include thermography, ultrasonography, magnetic resonance imaging, and computerized tomography, but none of these is believed to be as accurate as mammography. The first symptom noted is usually a lump or nodule in the breast tissue; however, dimpling of the breast skin or changes in the nipple may be noted before a lump is found. Diagnosis of a malignant tumor is confirmed by biopsy.
As with other forms of cancer, early detection and prompt treatment of malignancy of the breast are the keys to eradication of the disease. Studies have shown that breast self-examination has contributed to earlier detection and improved survival rates. It should be done monthly; more than 90 percent of breast cancers are discovered by the patients themselves either by chance or by routine self-examination. The American Cancer Society reports that only about 69 percent of women polled in the past had done self-examination at any time during the past year and less than 29 percent did it routinely each month.
Screening should begin by age 40 and should consist of a clinical examination every year and screening mammography every one or two years. Beginning at age 50, both the clinical examination and the mammography should be done once a year. mammography is considered to be the best diagnostic method for early detection when tumors are small and not readily found by palpation. Other diagnostic techniques include thermography, ultrasonography, magnetic resonance imaging, and computerized tomography, but none of these is believed to be as accurate as mammography. The first symptom noted is usually a lump or nodule in the breast tissue; however, dimpling of the breast skin or changes in the nipple may be noted before a lump is found. Diagnosis of a malignant tumor is confirmed by biopsy.
Treatment. Options for treatment of breast cancer are based on the clinical stage of the disease when first diagnosed or when re-evaluated. Formerly, the most common procedure was radical mastectomy. However, improvements in irradiation equipment and procedures, alternative surgical techniques that are less mutilating, and more active participation of patients in making decisions about the mode of therapy have all resulted in significant changes in the treatment of breast cancer.
Additional information can be obtained by calling the National Cancer Institute's Cancer Information Service Hotline at 1-800-4-CANCER.
Additional information can be obtained by calling the National Cancer Institute's Cancer Information Service Hotline at 1-800-4-CANCER.
chicken breast pectus carinatum.
funnel breast pectus excavatum.
pigeon breast pectus carinatum.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
Statistics BC is the most common CA in women; occurs in 12% of all US women, killing 3.5%—it is the leading COD in women age 40–55; in Japan, BC is 1/5 as common as it is in the US; it has doubled from 1930s to 1990s—± 55 to 105/100,000
Statistics Incidence: 450/100,000/year, age 75, US; mortality 125/100,000/year, age 75
Diagnosis Self-, doctor examination, mammography, ultrasonography, biopsy
Surveillance The American Cancer Society recommends a baseline mammogram at age 35 to 40; between 41 and 50, every other year, after age 50, annually; the thicker the bone, the greater the risk of BC; cause unknown, related to use of postmenopausal estrogens; ever active smokers have an odds ratio of 2.0 for breast CA, when compared to never active, never passive smokers
Risk factors Breast feeding—6 months—decreases risk of BC; lactation and breast feeding before age 20 is associated with a RR of 0.54
Susceptibility genes BRCA1, BRCA2, genes for Li-Fraumeni syndrome, Cowden disease, Muir-Torre syndrome, ataxia-telangiectasia predispose to breast CA; such genes account for 1/5 of breast CA
Chemotherapy Maximum effect with early treatment and maximum tolerable doses with cyclophosphamide, doxorubicin, fluorouracil
Surveillance Early detection, monthly breast self-examination, mammography at age-appropriate intervals
Therapeutic trends 1985–1993 Breast-conserving therapy, 31% 54%; axillary node dissection 52% 40%; RT 38% 54%
Segen's Medical Dictionary. © 2012 Farlex, Inc. All rights reserved.
breast cancer
Oncology An uncontrolled growth of abnormal breast tissue, usually epithelial in nature Statistics BC is the most common CA in ♀; occurs in 12% of all US ♀, killing 3.5%–it is the leading COD in ♀ age 40-55; in Japan, BC is1⁄5 as common as the US, but there has doubled from the mid-1930s to 1990s–± 55 to 105/105 StatisticsDeaths/Newly diagnosed44.5/185.7 Diagnosis Self- and physician examination, mammography, ultrasonography, biopsy Risk factors Breast feeding–≥ 6 months ↓ risk of BC; lactation and breast feeding before age 20 is associated with a RR of 0.54 Chemotherapy Maximum effect with early treatment and maximum tolerable doses with cyclophosphamide, doxorubicin, fluorouracil Surveillance Early detection, monthly breast self-examination, mammography at age-appropriate intervals Therapeutic trends 1985-1993 Breast-conserving therapy, 31%→54%; axillary node dissection 52%→40%; RT 38%→54%. See BRCA1, BRCA2.Breast cancer staging
- Stage I
- Cancer ≤ 2 cms; no spread outside the breast
- Stage II
- One of following– cancer ≤ 2 cm–spread to the axillary lymph nodes, or can cer of 2 to 5 cm that may/may not have spread to axillary lymph nodes, orcancer ≥ 5 cm without spread to axillary lymph nodes
- Stage III
-
- Defined by either 1. ≤ 5 cm and + axillary lymph nodes, which have grown into each other or into other structures and are attached to them, or 2. ≥ 5 cm and spread to axillary lymph nodes
- Cancer has spread to tissues near the breast–skin, chest wall, including the ribs and the muscles in the chest, or has spread to lymph nodes inside the chest wall along the breast bone
- Stage IV
- Cancer has metastasized, most often to bone, lungs, liver, or brain or has spread locally to skin and lymph nodes inside the neck, near the collarbone
McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
breast cancer
The commonest form of cancer in women, affecting about 1 in 12 women in Britain. Early breast cancer hardly ever causes pain and the only sign is a slowly growing lump. Later signs are distortion of the normal breast contour by skin dimpling, indrawing of the nipple, bleeding from the nipple, an orange-skin appearance (peau d'orange) of the breast skin, and rubbery, firm, easily felt lymph nodes in the armpit. Mammography for non-dense breast tissue and ultrasound scanning for dense tissue are the most effective screening methods. Most cases are treated by lumpectomy and radiotherapy or chemotherapy. Chemotherapy is an integral part of the management of resected node-positive cancer. Various combinations of drugs such as doxorubicin, cyclophosphamide and the taxane paclitaxel are used.Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005
Patient discussion about breast cancer
Q. what is inflamatory breast cancer?
A. It's a type of breast cancer that presents as an indurated, or hardened, red and edematous skin over the breast. It's considered an advanced cancer, and in most times when it's diagnosed there are cancer cells in the lymph nodes in the armpit (axilla) or metastases elsewhere in the body. It may be mistaken with infection of the breast.
You can read more here: http://en.wikipedia.org/wiki/Inflammatory_breast_cancer
You can read more here: http://en.wikipedia.org/wiki/Inflammatory_breast_cancer
Q. what are the risks for breast cancer?
A. Mainly exposure to estrogen, the female sex hormone, without progesterone, the other sex hormone to oppose it: younger age at the beginning of menses, older age of menopause, not being pregnant at all, older age at first pregnancy, hormonal replacement therapy (somewhat controversial). Also first degree relatives with breast or ovarian cancer, and specific mutations (such as BRCA1 or 2).
These are the major ones. You may find more info here: http://www.nlm.nih.gov/medlineplus/breastcancer.html
These are the major ones. You may find more info here: http://www.nlm.nih.gov/medlineplus/breastcancer.html
Q. Is it a breast cancer? My cousin, 30/female. She says that while she do some heavy work her right side breast is paining heavily. I am scared, whether is it a symptom of a breast cancer or something else. I like to help & comfort her?
A. Wow! quite a hot discussion in here..
I will say, what lixurion shared to us here is probably something new for all of us, and we need to consider it as additional knowledge,
BUT I will also encourage darwin to help his cousin to check her right breast to a doctor (maybe even an oncologist). If you agree with lixurion, then your oncologist should be able to detect the lump, and if it is needed, the doctor will do Fine Needle Aspiration to check it. Or if the effect of mammography is that bad, your doctor still can use ultrasound to check the inner tissue of her right breast.
The earlier a breast cancer is detected, the better the outcome result will be..
More discussions about breast cancerI will say, what lixurion shared to us here is probably something new for all of us, and we need to consider it as additional knowledge,
BUT I will also encourage darwin to help his cousin to check her right breast to a doctor (maybe even an oncologist). If you agree with lixurion, then your oncologist should be able to detect the lump, and if it is needed, the doctor will do Fine Needle Aspiration to check it. Or if the effect of mammography is that bad, your doctor still can use ultrasound to check the inner tissue of her right breast.
The earlier a breast cancer is detected, the better the outcome result will be..
This content is provided by iMedix and is subject to iMedix Terms. The Questions and Answers are not endorsed or recommended and are made available by patients, not doctors.