pyloric
[pi-lor´ik]pertaining to the pylorus or to the pyloric part of the stomach.
pyloric stenosis obstruction of the pyloric orifice of the stomach; it may be congenital, as in hypertrophic pyloric stenosis, or acquired, due to peptic ulceration or prepyloric carcinoma.
The initial symptom is vomiting, mild at first but becoming increasingly more forceful. It can occur both during and after feedings. Diagnosis may be confirmed by x-ray examination using a barium meal.
Treatment is usually surgical, involving longitudinal splitting of the muscle (pyloromyotomy).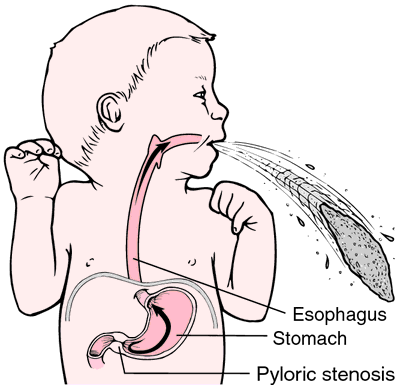
The initial symptom is vomiting, mild at first but becoming increasingly more forceful. It can occur both during and after feedings. Diagnosis may be confirmed by x-ray examination using a barium meal.
Treatment is usually surgical, involving longitudinal splitting of the muscle (pyloromyotomy).

Congenital pyloric stenosis. The abnormal narrowing of the opening of the pylorus causes episodes of projectile vomiting. From Frazier et al., 2000.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
py·lor·ic
(pī-lōr'ik),Relating to the pylorus.
Farlex Partner Medical Dictionary © Farlex 2012
pyloric
(pī-lôr′ĭk, pĭ-)adj.
Of or relating to the pylorus.
The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved.
py·lor·ic
(pī-lōr'ik)Relating to the pylorus.
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
pyloric
of or relating to that end of the vertebrate stomach which opens into the intestine. The other end is called the cardiac area of the stomach.Collins Dictionary of Biology, 3rd ed. © W. G. Hale, V. A. Saunders, J. P. Margham 2005