anemia
[ah-ne´me-ah]a condition in which there is reduced delivery of oxygen to the tissues; it is not actually a disease but rather a symptom of any of numerous different disorders and other conditions. The World Health Organization has defined anemia as a hemoglobin concentration below 7.5 mmol/L (12 g/dL) in women and below 8.1 mmol/L (13 g/dL) in men.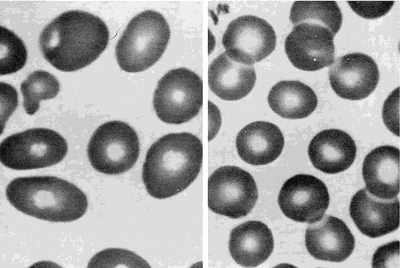
Some types of anemia are named for the factors causing them: poor diet (nutritional anemia), excessive blood loss (hemorrhagic anemia), congenital defects of hemoglobin (hypochromic anemia), exposure to industrial poisons, diseases of the bone marrow (aplastic anemia and hypoplastic anemia), or any other disorder that upsets the balance between blood loss through bleeding or destruction of blood cells and production of blood cells. Anemias can also be classified according to the morphologic characteristics of the erythrocytes, such as size (microcytic, macrocytic, and normocytic anemias) and color or hemoglobin concentration (hypochromic anemia). A type called hypochromic microcytic anemia is characterized by very small erythrocytes that have low hemoglobin concentration and hence poor coloration. Data used to identify anemia types include the erythrocyte indices: (1) mean corpuscular volume (MCV), the average erythrocyte volume; (2) mean corpuscular hemoglobin (MCH), the average amount of hemoglobin per erythrocyte; and (3) mean corpuscular hemoglobin concentration (MCHC), the average concentration of hemoglobin in erythrocytes. adj., adj ane´mic.
Activity intolerance is a common problem for patients with anemia. Physical activity increases demand for oxygen, but if there are not enough circulating erythrocytes to provide sufficient oxygen, patients become physically weak and unable to engage in normal physical activity without experiencing profound fatigue. This can result in some degree of self-care deficit as the fatigue interferes with the patient's ability to carry on regular or enjoyable activities.

Peripheral blood smears from a patient with megaloblastic anemia (left) and from a normal subject (right), both at the same magnification. The smear from the patient shows variation in the size and shape of erythrocytes and the presence of macro-ovalocytes. From Goldman and Bennett, 2000.
Some types of anemia are named for the factors causing them: poor diet (nutritional anemia), excessive blood loss (hemorrhagic anemia), congenital defects of hemoglobin (hypochromic anemia), exposure to industrial poisons, diseases of the bone marrow (aplastic anemia and hypoplastic anemia), or any other disorder that upsets the balance between blood loss through bleeding or destruction of blood cells and production of blood cells. Anemias can also be classified according to the morphologic characteristics of the erythrocytes, such as size (microcytic, macrocytic, and normocytic anemias) and color or hemoglobin concentration (hypochromic anemia). A type called hypochromic microcytic anemia is characterized by very small erythrocytes that have low hemoglobin concentration and hence poor coloration. Data used to identify anemia types include the erythrocyte indices: (1) mean corpuscular volume (MCV), the average erythrocyte volume; (2) mean corpuscular hemoglobin (MCH), the average amount of hemoglobin per erythrocyte; and (3) mean corpuscular hemoglobin concentration (MCHC), the average concentration of hemoglobin in erythrocytes. adj., adj ane´mic.
Symptoms. Mild degrees of anemia often cause only slight and vague symptoms, perhaps nothing more than easy fatigue or a lack of energy. As the condition progresses, more severe symptoms may be experienced, such as shortness of breath, pounding of the heart, and a rapid pulse; these are caused by the inability of anemic blood to supply the body tissues with enough oxygen. Pallor, particularly in the palms of the hands, the fingernails, and the conjunctiva (the lining of the eyelids), may also indicate anemia. In very advanced cases, swelling of the ankles and other evidence of heart failure may appear.
Common Causes of Anemia. Loss of Blood (Hemorrhagic Anemia): If there is massive bleeding from a wound or other lesion, the body may lose enough blood to cause severe and acute anemia, which is often accompanied by shock. Immediate transfusions are generally required to replace the lost blood. Chronic blood loss, such as excessive menstrual flow, or slow loss of blood from an ulcer or cancer of the gastrointestinal tract, may also lead to anemia. These anemias disappear when the cause has been found and corrected. To help the blood replenish itself, the health care provider may prescribe medicines containing iron, which is necessary to build hemoglobin, and foods with high iron content, such as kidney and navy beans, liver, spinach, and whole wheat bread.
Dietary Deficiencies and Abnormalities of Red Blood Cell Production (Nutritional Anemia, Aplastic Anemia, and Hypoplastic Anemia): Anemia may develop if the diet does not provide enough iron, protein, vitamin B12, and other vitamins and minerals needed in the production of hemoglobin and the formation of erythrocytes. The combination of poor diet and chronic loss of blood makes for particular susceptibility to severe anemia. Anemias associated with folic acid deficiency are very common.
Excessive Destruction of Red Blood Cells (hemolytic anemia): Anemia may also develop related to hemolysis due to trauma, chemical agents or medications (toxic hemolytic anemia), infectious disease, isoimmune hemolytic reactions, autoimmune disorders, and the paroxysmal hemoglobinurias.
Dietary Deficiencies and Abnormalities of Red Blood Cell Production (Nutritional Anemia, Aplastic Anemia, and Hypoplastic Anemia): Anemia may develop if the diet does not provide enough iron, protein, vitamin B12, and other vitamins and minerals needed in the production of hemoglobin and the formation of erythrocytes. The combination of poor diet and chronic loss of blood makes for particular susceptibility to severe anemia. Anemias associated with folic acid deficiency are very common.
Excessive Destruction of Red Blood Cells (hemolytic anemia): Anemia may also develop related to hemolysis due to trauma, chemical agents or medications (toxic hemolytic anemia), infectious disease, isoimmune hemolytic reactions, autoimmune disorders, and the paroxysmal hemoglobinurias.
Patient Care. Assessment of patients with some form of anemia will depend to some extent on the specific type of blood dyscrasia presented. In general, these patients do share some common problems requiring special assessment skills and interventions. Anemia can affect many different body systems
(see table). Although pallor of the skin is a sign of anemia, it is not the most reliable sign; many other factors can affect complexion and skin color. Jaundice of the skin and sclera can occur as a result of hemolysis and the release of bilirubin into the blood stream, where it eventually finds its way into the skin and mucous membranes. (See also jaundice.) Bleeding under the skin and bruises in response to the slightest trauma often are present in anemic and leukemic patients. A bluish tint to the skin (cyanosis) can indicate hypoxia due to inadequate numbers of oxygen-bearing erythrocytes.Activity intolerance is a common problem for patients with anemia. Physical activity increases demand for oxygen, but if there are not enough circulating erythrocytes to provide sufficient oxygen, patients become physically weak and unable to engage in normal physical activity without experiencing profound fatigue. This can result in some degree of self-care deficit as the fatigue interferes with the patient's ability to carry on regular or enjoyable activities.
acute posthemorrhagic anemia hemorrhagic anemia.
aplastic anemia see aplastic anemia.
autoimmune hemolytic anemia (AIHA) an acquired disorder characterized by hemolysis due to the production of autoantibodies against one's own red blood cell antigens.
Blackfan-Diamond anemia congenital hypoplastic anemia (def. 1).
congenital hypoplastic anemia
idiopathic progressive anemia occurring in the first year of life, without leukopenia and thrombocytopenia; it is due to an isolated defect in erythropoiesis and is unresponsive to hematinics, requiring multiple blood transfusions to sustain life. For those responding to steroid therapy the prognosis is good. Called also Blackfan-Diamond anemia or syndrome, Diamond-Blackfan anemia or syndrome, and erythrogenesis imperfecta.
Fanconi's syndrome (def. 1).
Cooley's anemia tthalassemia major.
deficiency anemia nutritional anemia.
Diamond-Blackfan anemia congenital hypoplastic anemia (def. 1).
drug-induced hemolytic anemia (drug-induced immune hemolytic anemia) a form of immune hemolytic anemia induced by the taking of drugs, involving one of four different mechanisms:
Immune complex problems: Ingestion of any of a large number of drugs is followed by immunization and the formation of a soluble drug–anti-drug complex that adsorbs nonspecifically to the erythrocyte surface.
Drug absorption: Drugs bind firmly to erythrocyte membrane proteins, inducing the formation of specific antibodies; the drug most commonly associated with this mechanism is penicillin.
Membrane modification: A nonimmunologic mechanism whereby the drug involved is able to modify erythrocytes so that plasma proteins can bind to the membrane.
Autoantibody formation: Methyldopa (Aldomet) induces the production of autoantibodies that recognize erythrocyte antigens and are serologically indistinguishable from those seen in patients with warm autoimmune hemolytic anemia.
Immune complex problems: Ingestion of any of a large number of drugs is followed by immunization and the formation of a soluble drug–anti-drug complex that adsorbs nonspecifically to the erythrocyte surface.
Drug absorption: Drugs bind firmly to erythrocyte membrane proteins, inducing the formation of specific antibodies; the drug most commonly associated with this mechanism is penicillin.
Membrane modification: A nonimmunologic mechanism whereby the drug involved is able to modify erythrocytes so that plasma proteins can bind to the membrane.
Autoantibody formation: Methyldopa (Aldomet) induces the production of autoantibodies that recognize erythrocyte antigens and are serologically indistinguishable from those seen in patients with warm autoimmune hemolytic anemia.
Fanconi's anemia (Fanconi's hypoplastic anemia) Fanconi's syndrome (def. 1).
hemolytic anemia see hemolytic anemia.
hemorrhagic anemia anemia caused by the sudden and acute loss of blood; called also acute posthemorrhagic anemia.
hypochromic anemia anemia in which the decrease in hemoglobin is proportionately much greater than the decrease in number of erythrocytes.
hypochromic microcytic anemia any anemia with microcytes that are hypochromic (reduced in size and in hemoglobin content); the most common type is iron deficiency anemia.
hypoplastic anemia anemia due to incapacity of blood-forming organs.
immune hemolytic anemia an acquired hemolytic anemia in which a hemolytic response is caused by isoantibodies or autoantibodies produced on exposure to drugs, toxins, or other antigens. See also autoimmune hemolytic anemia, drug-induced immune hemolytic anemia, and erythroblastosis fetalis.
iron deficiency anemia a type of hypochromic microcytic anemia that results from the presence of greater demands on stored iron than can be met, usually because of chronic blood loss, dietary deficiency, or defective absorption; it is characterized by low or absent iron stores, low serum iron concentration, low transferrin saturation, elevated transferrin (total iron-binding capacity), and low hemoglobin concentration or hematocrit. Iron deficiency anemia is the most common nutritional disorder in the United States.
macrocytic anemia anemia characterized by macrocytes (erythrocytes much larger than normal).
Mediterranean anemia thalassemia major.
megaloblastic anemia any of various anemias characterized by the presence of megaloblasts in the bone marrow or blood; the most common type is pernicious anemia.
microangiopathic hemolytic anemia thrombotic thrombocytopenic purpura.
microcytic anemia anemia characterized by microcytes (erythrocytes smaller than normal); see also hypochromic microcytic anemia and microcythemia.
myelopathic anemia (myelophthisic anemia) leukoerythroblastosis.
normochromic anemia that in which the hemoglobin content of the red blood cells is in the normal range.
normocytic anemia anemia characterized by proportionate decrease in hemoglobin, packed red cell volume, and number of erythrocytes per cubic millimeter of blood.
nutritional anemia anemia due to a deficiency of an essential substance in the diet, which may be caused by poor dietary intake or by malabsorption; called also deficiency anemia.
pernicious anemia see pernicious anemia.
sickle cell anemia see sickle cell anemia.
sideroachrestic anemia (sideroblastic anemia) any of a heterogenous group of acquired and hereditary anemias with diverse clinical manifestations, commonly characterized by large numbers of sideroblasts in the bone marrow, ineffective erythropoiesis, variable proportions of hypochromic erythrocytes in the peripheral blood, and usually increased levels of tissue iron.
spur cell anemia anemia in which the erythrocytes are acanthocytes (spur cells) and are destroyed prematurely, primarily in the spleen; it is an acquired form occurring in severe liver disease in which there is increased serum cholesterol and increased uptake of cholesterol into the erythrocyte membrane, causing the abnormal shape.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
a·ne·mi·a
(ă-nē'mē-ă),Any condition in which the number of red blood cells/mm3, the amount of hemoglobin in 100 mL of blood, and/or the volume of packed red blood cells/100 mL of blood are less than normal; clinically, generally pertaining to the concentration of oxygen-transporting material in a designated volume of blood, in contrast to total quantities as in oligocythemia, oligochromemia, and oligemia. Anemia is frequently manifested by pallor of the skin and mucous membranes, shortness of breath, palpitations of the heart, soft systolic murmurs, lethargy, and tendency to fatigue.
[G. anaimia, fr. an- priv. + haima, blood]
Farlex Partner Medical Dictionary © Farlex 2012
anemia
alsoanaemia
(ə-nē′mē-ə)n.
A pathological deficiency in the oxygen-carrying component of the blood, measured in unit volume concentrations of hemoglobin, red blood cell volume, or red blood cell number.
The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved.
anaemia
A condition characterised by decreased red cells or haemoglobin in the blood, resulting in decreased O2 in peripheral tissues. Anaemias are divided into various groups based on cause—e.g., iron deficiency anaemia, megaloblastic anaemia (due to decreased vitamin B12 or folic acid) or aplastic anaemia (where RBC precursors in the bone marrow are depleted).Clinical findings
Fatigability, pallor, palpitations, shortness of breath.
Anaemia classifications
Morphology
Macrocytic
• Megaloblastic anaemia:
– Vitamin B12 deficiency;
– Folic acid deficiency.
Microcytic hypochromic
• Iron-deficiency anaemia;
• Hereditary defects;
• Sickle cell anaemia;
• Thalassemia;
• Other heamoglobinopathies.
Normocytic
• Acute blood loss;
• Haemolysis;
• BM failure;
• Anaemia of chronic disease;
• Renal failure.
Aetiology
Deficiency
• Iron;
• Vitamin B12;
• Folic acid;
• Pyridoxine;
Central (due to BM failure)
• Anaemia of chronic disease;
• Anaemia of senescence;
• Malignancy:
– BM replacement by tumour;
– Toxicity due to chemotherapy;
– Primary BM malignancy, e.g., leukaemia.
Peripheral
• Haemorrhage;
• Haemolysis.
Segen's Medical Dictionary. © 2012 Farlex, Inc. All rights reserved.
anemia
Hematology A condition characterized by ↓ RBCs or Hb in the blood, resulting in ↓ O2 in peripheral tissues Clinical Fatigability, pallor, palpitations, SOB; anemias are divided into various groups based on cause–eg, iron deficiency anemia, megaloblastic anemia–due to ↓ vitamin B12 or folic acid, or aplastic anemia–where RBC precursors in BM are 'wiped out'. See Anemia of chronic disease, Anemia of investigation, Anemia of prematurity, Aplastic anemia, Arctic anemia, Autoimmune hemolytic anemia, Cloverleaf anemia, Congenital dyserythropoietic anemia, Dilutional anemia, Dimorphic anemia, Drug-induced immune hemolytic anemia, Fanconi anemia, Hemolytic anemia, Idiopathic sideroblastic anemia, Immune anemia, Iron-deficiency anemia, Juvenile pernicious anemia, Macrocytic anemia, Megaloblastic anemia, Microcytic anemia, Myelophthisic anemia, Neutropenic colitis with aplastic anemia, Nonimmune hemolytic anemia, Pseudoanemia, Refractory anemia with excess blasts, Sickle cell anemia, Sideroblastic anemia, Sports anemia.General groups of anemia
- Morphology
- Macrocytic
- Megaloblastic anemia
- Vitamin B12deficiency
- Folic acid deficiency
- Microcytic hypochromic
-
- Iron-deficiency anemia
- Hereditary defects
- Sickle cell anemia
- Thalassemia
- Other hemoglobinopathies
- Normocytic
-
- Acute blood loss
- Hemolysis
- BM failure
- Anemia of chronic disease
- Renal failure
- Etiology
- Deficiency
-
- Iron
- Vitamin B12
- Folic acid
- Pyridoxine
- Central–due to BM failure
-
- Anemia of chronic disease
- Anemia of senescence
- Malignancy
- BM replacement by tumor
- Toxicity due to chemotherapy
- Primary BM malignancy, eg leukemia
- Peripheral
-
- Hemorrhage
- Hemolysis
McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
a·ne·mi·a
(ă-nē'mē-ă)Any condition in which the number of red blood cells per mm3, the amount of hemoglobin in 100 mL of blood, or the volume of packed red blood cells per 100 mL of blood is less than normal; clinically, generally pertaining to the concentration of oxygen-transporting material in a designated volume of blood. It is frequently manifested by pallor of the skin and mucous membranes, shortness of breath, palpitations of the heart, soft systolic murmurs, lethargy, and fatigability.
Synonym(s): anaemia.
Synonym(s): anaemia.
[G. anaimia, fr. an- priv. + haima, blood]
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
Anemia
A condition in which there is an abnormally low number of red blood cells in the bloodstream. Major symptoms are paleness, shortness of breath, unusually fast or strong heart beats, and tiredness.
Mentioned in: Antianemia Drugs, Babesiosis, Barbiturates, Bone Marrow Transplantation, Colon Cancer, Coombs' Tests, Dyspepsia, Erythroblastosis Fetalis, Erythropoietin Test, Fetal Hemoglobin Test, Fifth Disease, Graft-vs.-Host Disease, Hairy Cell Leukemia, Hematocrit, Hemoglobin Test, Histiocytosis X, Hookworm Disease, Iron Tests, Jaundice, Leeches, Malabsorption Syndrome, Malnutrition, Multiple Myeloma, Myelofibrosis, Nonsteroidal Anti-Inflammatory Drugs, Pernicious Anemia, Platelet Function Disorders, Polymyalgia Rheumatica, Pyruvate Kinase Deficiency, Radiation Therapy, Rectal Cancer, Red Blood Cell Indices, Restless Legs Syndrome, Reticulocyte Count, Sickle Cell Disease, Starvation, Stomach Cancer, Sulfonamides, Temporal Arteritis, Thalassemia, 2,3-Diphosphoglycerate Test, Urinary Anti-Infectives, Uterine Fibroid Embolization, Uterine Fibroids, Waldenström's Macroglobulinemia, Wilson Disease, Wiskott-Aldrich Syndrome
Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.
a·ne·mi·a
(ă-nē'mē-ă)Any condition in whichthe number of red blood cells/mm3, the amount of hemoglobin in 100 mL of blood, and/or the volume of packed red blood cells/100 mL of blood are less than normal; frequently manifested by pallor of the skin and mucous membranes, shortness of breath, palpitations of the heart, soft systolic murmurs, lethargy, and tendency to fatigue.
Synonym(s): anaemia.
Synonym(s): anaemia.
[G. anaimia, fr. an- priv. + haima, blood]
Medical Dictionary for the Dental Professions © Farlex 2012
Patient discussion about Anemia
Q. What is the Treatment for Anemia? I would like to know what are the possible treatments for anemia?
A. The first step in treating anemia, is discovering the cause for it. By a series of simple blood tests it is easy to discover iron defficiency, folic acid defficiency and vitamin B12 defficiency anemia, all which can be treated with oral supplements or a change of nutrition. Anemia that is associated with rectal bleeding should be further investigated, because it is often the first sign of colon polyps or colon cancer. Colonoscopy is then recommended.
Q. What are the Symptoms of Anemia? Lately I've been feeling very tired. My friend suggested I might be anemic. What are the major symptoms of anemia?
A. The symptoms of anemia vary according to the type of anemia, the underlying cause, and any underlying health problems. Anemia may be associated with other medical conditions such as hemorrhage, ulcers, menstrual problems or cancer -- and specific symptoms of those conditions may be noticed first.
The body also has a remarkable ability to compensate for early anemia. If your anemia is mild or developed over a long period of time, you may not notice any symptoms. Symptoms common to many types of anemia include the following:
Easy fatigue and loss of energy
Unusually rapid heart beat, particularly with exercise
Shortness of breath and headache, particularly with exercise
Difficulty concentrating
Dizziness
Pale skin
Leg cramps
Insomnia
Hope this helps.
http://www.webmd.com/a-to-z-guides/understanding-anemia-symptoms
The body also has a remarkable ability to compensate for early anemia. If your anemia is mild or developed over a long period of time, you may not notice any symptoms. Symptoms common to many types of anemia include the following:
Easy fatigue and loss of energy
Unusually rapid heart beat, particularly with exercise
Shortness of breath and headache, particularly with exercise
Difficulty concentrating
Dizziness
Pale skin
Leg cramps
Insomnia
Hope this helps.
http://www.webmd.com/a-to-z-guides/understanding-anemia-symptoms
Q. What is the Definition of Anemia? My doctor told me I have anemia, based on my latest blood tests. What is anemia?
A. In laymans terms it is low iron. Most women get it sometime in their lives due to menstration and other factors. You need to increase your iron intake. Lots of beets, beans, spinich, and lots of other foods can help.
More discussions about AnemiaThis content is provided by iMedix and is subject to iMedix Terms. The Questions and Answers are not endorsed or recommended and are made available by patients, not doctors.