sac
[sak]air s's (alveolar s's) the spaces into which the alveolar ducts open distally, and with which the alveoli communicate; see also lung.
amniotic sac the sac formed by the amnion, enclosing the fetus suspended in amniotic fluid; popularly known as the bag of waters.
conjunctival sac the potential space, lined by conjunctiva, between the eyelids and the eyeball.
endolymphatic sac the blind, flattened cerebral end of the endolymphatic duct.
hernial sac the peritoneal pouch that encloses protruding intestine.
lacrimal sac the dilated upper end of the nasolacrimal duct; see also lacrimal apparatus.
yolk sac the extraembryonic membrane connected with the midgut; in vertebrates below true mammals, it contains a yolk mass.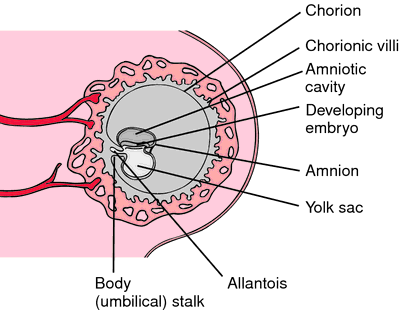

Yolk sac in a developing embryo. From Applegate, 2000.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
her·ni·al sac
the protruding envelope of peritoneum in a hernia.
Farlex Partner Medical Dictionary © Farlex 2012
her·ni·al sac
(hĕr'nē-ăl sak)The peritoneal envelope of a hernia.
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
hernial sac
A bag of PERITONEUM pushed through a hernial orifice and containing the loop of bowel or other body part that has herniated.Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005